

Understanding a Rare Zoonotic Virus Through Science, Not Fear
Recent media coverage surrounding hantavirus, particularly the Andes strain linked to South America, has generated unnecessary public anxiety while omitting critical scientific context. Hantaviruses are not new, mysterious, or rapidly emerging pathogens. They are a well-characterized family of rodent-borne RNA viruses that have been studied for decades.
The Andes strain has circulated in Argentina since at least 1995, with periodic outbreaks occurring in endemic regions where human exposure to infected rodents is known to occur. Reports from late 2025 documented approximately twenty deaths in Argentina, within the expected epidemiological pattern of a known regional disease.
The omnipresent media coverage suggests the possibility of a new public health crisis. The evidence does not support that conclusion.
Origins and Transmission
Hantaviruses are a family of negative-sense single-stranded RNA viruses carried by specific rodent species. In the United States, the primary strain is the Sin Nombre virus, carried by the deer mouse. Infection occurs almost exclusively through inhalation of aerosolized particles from rodent urine, droppings, or saliva in dusty, enclosed spaces. This is fundamentally different from viruses that spread efficiently person-to-person.
The Andes strain has circulated in Argentina since at least the mid-1990s. Recent ship-associated cases are most likely due to the known common mechanism of transmission, which is environmental contamination during boarding or provisioning — a sanitation and rodent-control issue, not a new contagious outbreak. It would not be good public relations for the cruise line to acknowledge rats on board but this is by far the most likely cause.
Debunking Person-to-Person Transmission Claims
Virtually every mainstream media commentator has accepted the narrative that the Andes strain of hantavirus spreads readily person-to-person in the community. This claim is being used to justify biosecurity measures and quarantines, including for passengers from the recent ship incident.
The evidence does not support efficient person-to-person transmission.
Nonetheless: the WHO locked passengers into their cabins … with infected rodents and ventilation system … fresh air on the deck is not permitted.
Let that sink in.
And feel incredibly grateful that the USA has “jumped ship” from the WHO.
The primary foundation for the P2P hypothesis is the Martínez et al. (2020) paper in the New England Journal of Medicine, which examined a 2018–2019 cluster in the small rural village of Epuyén, Argentina. That study relied on contact tracing, temporal clustering, and genetic similarity — but did not sample homes, dust, or buildings for rodent contamination. Environmental exposure was largely ruled out based on patient interviews rather than objective testing.
A more rigorous Toledo et al. (2022) systematic review in The Journal of Infectious Diseases examined all available evidence on human-to-human transmission of hantaviruses, including the Martínez papers. Their conclusion: The balance of evidence does not support person-to-person transmission of Andes virus. Most studies suffered from critical risk of bias, particularly the failure to rule out shared environmental exposure to infected rodent droppings.
In real-world observation from the recent ship cases:
- Dead bodies were kept aboard for days (a potential high-viral-load source).
- Passengers who deboarded early, are out with no apparent spread.
- Crew members, after weeks of exposure, continue their normal duties.
This is consistent with decades of data on hantaviruses: they are primarily or (more likely) exclusively rodent-borne, aerosolized from urine/droppings/dust, and require a sufficient infectious dose via inhalation. Claims of efficient community P2P spread are being driven by other motives — not by science.
Diagnosis and Clinical Presentation
Early hantavirus symptoms are nonspecific and may resemble influenza, COVID-19, gastrointestinal illness, or other viral syndromes.
Exposure history is — by far — the most important diagnostic clue. Clinicians evaluate whether a patient has had recent contact with rodent-infested areas, swept enclosed dusty spaces, spent time in cabins or barns, or traveled through endemic regions in the western United States or South America. Laboratory confirmation could involve PCR testing during early infection, although it is notoriously inaccurate especially with hantavirus. Thus serologic antibody testing is the most relevant test.
Early laboratory findings may include thrombocytopenia, hemoconcentration, atypical lymphocytes, and rapidly evolving pulmonary edema with relatively clear cardiac findings.
Distribution and Incidence
In the United States, hantavirus cases occur predominantly in western and southwestern states, particularly the Four Corners region: New Mexico, Arizona, Colorado, and Utah.
Cases have also occurred in Nevada, Montana, Wyoming, Oregon, Washington, Idaho, and Texas. Risk is strongly associated with rodent population density, environmental conditions, rural dust exposure, and the degree of human interaction with rodent habitats such as sheds, cabins, and agricultural structures.
Although the deer mouse is widespread throughout much of the United States, human disease incidence remains significantly higher in western and southwestern regions.
Since national surveillance began in 1993, the CDC has identified fewer than 1,000 confirmed U.S. cases.
Treatment and Early Therapeutic Research
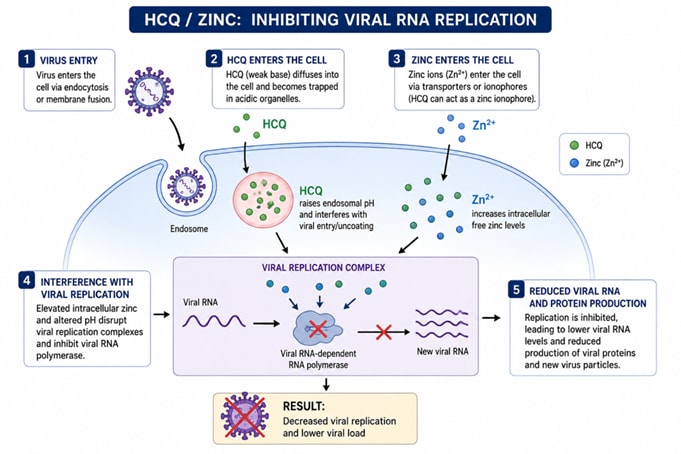
Hantaviruses are negative-sense single-stranded RNA viruses that, despite structural differences from viruses like SARS-CoV-2, depend on similar host cell machinery and intracellular transport pathways for replication. Both hydroxychloroquine (HCQ) and ivermectin (IVM) disrupt these pathways, resulting in strong antiviral benefits. Early in the infection, the virus relies heavily on its polymerase activity. Mechanistically, HCQ or Quercetin combined with zinc targets early viral entry and replication steps directly. Quercetin is over the counter and HCQ or ivermectin needs a prescription. If you would like to make a physician appointment to discuss hantavirus you can do this at GoldCare.com/AFLDS and a portion of that charge will be donated to AFLDS.
HCQ or Quercetin plus zinc blocks early viral entry and replication through several actions: it raises endosomal pH (hantaviruses require acidic conditions for entry), promotes intracellular zinc accumulation (zinc inhibits the viral RNA-dependent RNA polymerase enzyme needed for replication), and directly inhibits that polymerase. HCQ also helps modulate the immune response to reduce harmful inflammation and vascular leakage. Supporting evidence includes a 2021 peer-reviewed study in Frontiers in Cellular and Infection Microbiology, which tested chloroquine (a precursor to HCQ) against multiple hantaviruses, including Andes virus. When given before infection, it achieved 60% survival in hamsters (versus 0% in untreated controls) and demonstrated strong antiviral activity in vitro across hantavirus species. Zinc amplifies HCQ’s effects, while Vitamin D strengthens innate antiviral defenses and dampens excessive inflammation, and Vitamin C supports immune cell function, protects blood vessels, and helps counter cytokine storm and vascular damage.
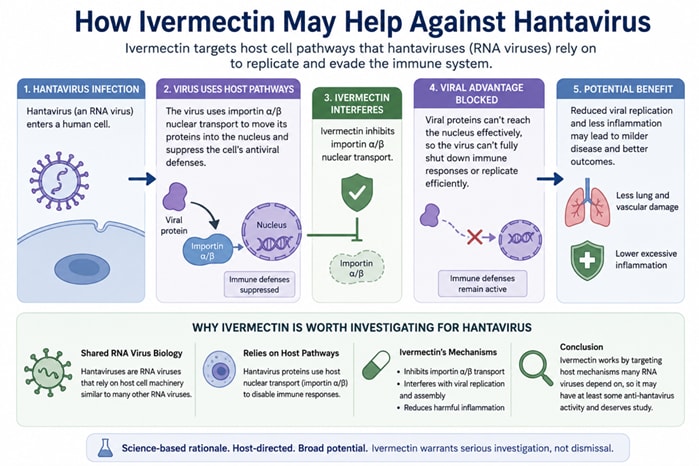
Ivermectin (IVM) acts more broadly on later intracellular replication stages. It inhibits importin α/β-mediated transport of viral proteins into the nucleus (a pathway hantaviruses use to weaken host antiviral defenses), interferes with viral protein transport and replication, and reduces inflammatory effects in the lungs. Ivermectin has a well-documented history of broad-spectrum antiviral activity against many RNA viruses (including dengue, Zika, West Nile, influenza, and SARS-CoV-2), as summarized in a 2020 systematic review by Heidary et al. and aggregated data across numerous studies.
Timing is critical. Treatment is most effective when started very early—during the exposure phase, at the end of incubation, or on the first day of fever/myalgia —when viral replication is dominant. In the later phase, disease is driven primarily by endothelial dysfunction and vascular leakage rather than high viral load, so endothelial stabilization and hemodynamic support become the priority. Early intervention with HCQ/zinc or IVM aims to reduce viral burden before this serious inflammatory/endothelial cascade becomes irreversible.
Environmental Prevention and Disinfection
Because hantavirus transmission is strongly linked to contaminated rodent environments, prevention remains the most effective strategy.
Recommended prevention measures include rodent exclusion and control, proper sanitation and environmental cleaning, avoiding aerosolization of contaminated dust during cleanup, and appropriate disinfectant use in contaminated areas.
Hypochlorous acid (HOCl) is an ancient and well-studied disinfectant with broad antimicrobial activity against bacteria, fungi, and many enveloped RNA viruses. Evidence supports the use of hypochlorous acid for environmental decontamination, surface disinfection, topical antimicrobial applications, and ongoing nasal and oral hygiene research. You can buy Curaclean here.
Separating Risk From Narrative
Hantavirus is a serious illness, but seriousness does not justify exaggeration.
The current evidence shows a known zoonotic disease with a rare pattern of human illness, clear environmental risk factors, and little to no evidence supporting sustained human-to-human transmission. Practical prevention strategies remain centered on sanitation, rodent control, and reducing environmental exposure.
As Dr. Pierre Kory recently observed about the current media surge:
“... 100,000 articles written around the world on Hantavirus in the last couple of days, and that's not typical...it seems to be driven by influencers...these patterns are anomalous...it's being driven by something.”
Fear-based communication distorts public understanding and undermines trust. Scientific literacy requires proportionality, context, and transparency.
Public Health Narratives and Institutional Trust
Public skepticism toward infectious disease narratives is highly rational given the government’s track record.
During the COVID-19 pandemic, major institutions (CDC, WHO, and others) suppressed information, mocked scientific inquiry, and aggressively pushed nonsensical ineffective policies such as masking, “shelter-in-place” and “six-foot social distancing”. Our government officials denied natural immunity, and misled the public on vaccine effectiveness. Scientific debate was discouraged or censored. The WHO under Director-General Tedros Adhanom Ghebreyesus (the first WHO chief without a medical degree and former leader of a leftist terrorist organization in his home country), faced widespread criticism for its handling of COVID-19.
Many observers note the decades-long control by the Chinese Communist Party over the WHO. These dynamics have fueled severe concerns about proposals such as the WHO Pandemic Treaty, which grants this international body led by the Chinese Communist Party significant authority over a nation’s sovereignty regarding its health policy and individual rights.
This has eroded trust, especially when the media and institutions dramatically exaggerate the threat of a rare, mostly environmentally transmitted zoonotic virus. The American people have learned to ask: Is this really proportional to the threat? Are government health officials pushing honest solutions like rodent control and proper cleaning — or are they once again using fear to expand their power?
Fear-based communication and disproportionate coverage have damaged public trust. Rebuilding confidence requires transparency, respect for scientific debate, accurate risk communication, and rejection of panic-driven policy.
Moving Forward With Scientific Clarity
Public health efforts should focus on accurate risk communication, environmental prevention, early clinical recognition, and rational scientific investigation of potential therapies.
A virus that has existed for decades should not be presented as an unexplained or uncontrollable threat simply because alarming narratives generate attention.
The American people deserve calm analysis rooted in evidence, not speculation designed to provoke fear.
A well-informed public is not fearful. It is prepared.